By Dr Rais Hussin / Dr Margarita Peredaryenko / Jason Loh / Ameen Kamal
The most recent research findings suggest that the SARS-CoV-2 Delta variant replicates at a much higher speed than the original virus resulting in a higher viral load and infectiousness earlier on. Hence the unprecedented speed and reach of Delta variant in population make staying ahead of the virus more challenging and essential.
First of all, the Delta variant spread places a higher demand on the system of finding, testing, tracing, isolating and supporting (FTTIS) for its aggressiveness–nearly real-time speed and scale.
Mass testing and fast tracing are still essential despite the high positivity rate (indicating pandemic management getting out of control). Quick early detection is still everything in preventing greater escalation of the spread and, importantly, higher death tolls. Furthermore, empirical evidence shows that robust and adequate FTTIS system can be traded for aggressive lockdowns.
Increased lab capacity, widespread utilization of rapid test kits, and Big Data are essential policy responses to speed up FTTIS. To capture a potentially large number of non-obvious exposures, the government should consider relooking the use of Bluetooth-powered near-contact detection functionality into the MySejahtera app.
Aggressive testing is crucial for yet another reason—early prevention of disease severity progression, which is perhaps the most pressing need in pandemic management and is still overlooked.
There are four distinct stages in COVID-19 disease progression: incubation, symptomatic stage, early pulmonary phase, and late pulmonary phase.
However, we can categorize these stages more broadly into two treatment-specific phases:
1. Active viral replication,
2. Dysregulated inflammatory response.
The prophylaxis, earliest detection of the second phase and its earlier treatment make a difference in the COVID-19 management outcome!
Notably, the second phase does not develop in all patients. In some patients, more likely than in others, the immune system fails to downregulate cytotoxic (proinflammatory) response.
One stream of research explains this inability through Vitamin D deficiency observed in severe COVID-19 patients with profound regularity. EMIR Research's earlier article "D-hammer option to flatten the curve" delved into the detailed science, strong empirical evidence and policy implications of this connection.
Another stream of COVID-19 frontier research begins to discover that the inflammatory phase develops as an autoimmune reaction to ACE2 receptors amply present in human lung and small intestine epithelium as well as in vascular endothelium. This leads to disruption of the epithelium and endothelium smoothness followed by blood coagulation, clotting and eventually pulmonary involvement.
COVID-19 Associated Coagulopathy (CAC) has been described as a "hypercoagulable" condition in many reports. According to Dugue and colleagues, CAC is an "emerging hallmark of the COVID-19 pandemic, contributing to macro- and microvascular complications". And CAC is the main reason behind "organizational pneumonia" (not viral or bacterial) observed in COVID-19 patients.
These findings carry profound implications for COVID-19 management as the treatment of severe inflammatory response, including organizational pneumonia, is well established through the use of corticosteroids and anticoagulants.
This led some researchers to posit timely and aggressive corticosteroids-anticoagulation regimen incorporated in the MATH+ protocol, as a critical disease progression prevention strategy.
The key paper describing MATH+ presents a rigorous review of scientific rationale and empirical evidence (including well-designed clinical trials in SARS-CoV, MERS, H1N1 and SARS-CoV-2) that underpins the protocol.
Remarkably, all MATH+ core therapies are highly familiar, low-cost, approved medications with well-established safety profiles.
According to proponents of MATH+, as the hospital treatment protocol for COVID-19 patients, early-stage interventions to support innate immune response (nutritional supplementation) alongside addressing autoimmune reaction (corticosteroids) and hypercoagulation (anticoagulants) are an essential part of disease management, and most importantly, prevention of disease progression.
Importantly, corticosteroids and anticoagulants should be started at the first signs of pulmonary involvement. Hence the general public must be well guided to seek immediate medical assistance at the earliest signs of pulmonary involvement.
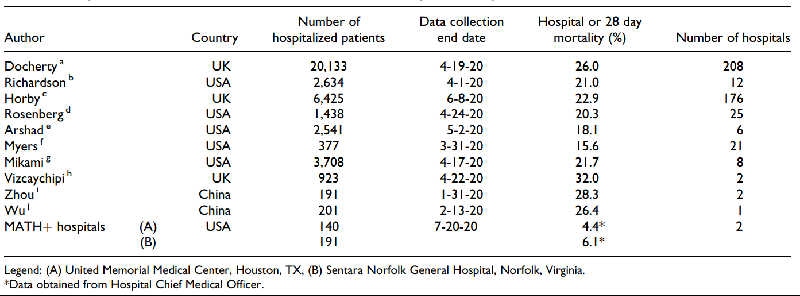
The table below (adopted from Kory et al.) demonstrates the remarkable results for mortality reduction by the MATH+ protocol practicing hospitals.
In contrast to MATH+, our current clinical management appears to suggest that no treatment is required for the patient at Category 3 except clinical observations to determine disease progression. However, the same document indicates that Category 3 patients already demonstrate signs of serious pulmonary involvement and, therefore, according to MATH+, should be started on steroids and anticoagulants.
The local protocol suggests only starting corticosteroids (dexamethosone and methylprednisolone) for Category 4 patients. This is likely because it is established that steroids use during viral replication could hamper natural antiviral activities of the body, therefore, working against it – increasing viral replication and worsening symptoms.
However, MATH+ proponents suggest that viral replication ends before entering the pulmonary phase, and one study indicates that corticosteroids use in the pulmonary phase does not inhibit viral clearing, while another study shows that it does not negatively impact specific type of antibodies production. Furthermore, a systematic meta-analytical review found that beyond day-9 of illness, none of the studies detected live viruses. This supports the notion that viral replication stops before entering the pulmonary phase in line with MATH+.
Also, in contrast to local protocol, MATH+ suggests using antivirals earlier—in the pre-pulmonary-involvement stage. In addition to antivirals, MATH+ recommends using vitamins such as Vitamin C and D early on.
There is no mention of vitamins in local protocols in any disease phases.
Vitamin C has been reported to assist in the production of interferons and decrease proinflammatory cytokines, both of which affect the body's antiviral response. Therefore, such nutritional supplementation must be provided in the early stages.
Increased disease progression may be associated with increased inflammatory responses by the body and it has been reported that cytokine storms may lead to even more proinflammatory cytokines and reactive oxygen species that lead to oxidative damage. In this scenario, it is reported that Vitamin C could work in concert with steroids to prevent oxidative damage to the steroid receptors.
This is why MATH+ recommends Vitamin C and D supplementation throughout all stages. In addition, there are other medications suggested under MATH+ such as thiamine, zinc, melatonin and other medications that could supplement current local protocols.
SARS-CoV-2 pathogenicity is complex, and the immune system requires multi-pronged support.
It is understood that the Ministry of Health (MOH) has conducted a review on micronutrients in COVID-19 management and concluded that more studies are needed to support the link between micronutrients intervention and COVID-19 patients' outcomes. However, EMIR Research's earlier article "D-hammer option to flatten the curve" strongly supports the notion with the most recent empirical evidence.
The above science-driven policy recommendations are crucial to reduce pressure on the healthcare system capacity and reduce the mortality rate. MATH+ protocol deserve the health authorities’ attention.
Furthermore, private hospitals involvement could help to scale the success. The current arrangement with the Association of Private Hospitals Malaysia's (APHM) is expected to continue beyond the Emergency.
Firstly, the government should fully subsidize the costs of the private sector.
At the same time, subsidies should be accompanied by enforcement of price controls.
The Ministry of Domestic Trade & Consumer Affairs should work closely with MOH to monitor for excessive charges and intervene by enforcing pre-existing caps by use of the Price Control and Anti-Profiteering (Mechanism to Determine Unreasonably High Profit for Goods) Regulations 2016 made under the Price Control Anti-Profiteering Act (2011).
Concerning other hospital fees like test charges and drug charges, MOH should also extend application under the Thirteenth Schedule of the Private Facilities and Services (Private Hospitals and Other Private Healthcare Facilities) Regulations 2006 of the Private Healthcare Facilities and Services Act (1998). This is to prevent cost-escalation due to e.g. "high demand", "supply constraints", "double workload", etc.
Secondly, other arrangements that mimic the provisions of the Emergency Ordinance should also be made.
Empty fields should be the site of makeshift buildings, which should allow for better ventilation. Otherwise, modular/prefabricated buildings based on Industrialized Building Systems (IBS) should be heavily considered. Such construction methods can definitively preempt concerns of clusters forming at the sites since building materials and building blocks are manufactured off-site and only brought on-site for modular assembling.
Empty buildings should be quickly converted into temporary COVID-19 hospitals, which would also alleviate the burden on the private healthcare sector. These empty buildings, if possible, can then become fully-fledged and permanent hospitals in the future – with the capacity to absorb contract medical officers/doctors on a permanent basis. With this, the government saves on construction costs whilst focusing on upgrading and retrofitting (for ventilation and air filtration purposes).
Excess supply of ventilators and oxygen tanks can then be reallocated to these previously unused/under-used sites that now have been transformed into makeshift or temporary COVID-19 hospitals.
Speed and scale of proactive early intervention are keys to managing the current situation – simultaneously balancing containment, economic openness and alleviating the healthcare burden.
(Dr Rais Hussin, Dr Margarita Peredaryenko, Jason Loh and Ameen Kamal are part of the research team of EMIR Research, an independent think tank focused on strategic policy recommendations based on rigorous research.)
ADVERTISEMENT
ADVERTISEMENT